AUDIOGRAM – INTERPRETING RESULTS
An audiogram represents an individual’s hearing ability by frequency (pitch) and intensity (volume). The softest sounds that a person can hear at a particular frequency is called their hearing threshold. This is usually represented by markings on their graph; red represents the right ear and blue represents the left.
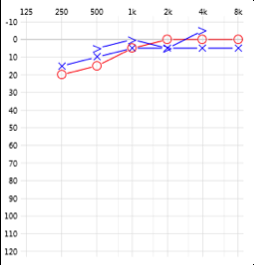
Hearing within normal limits.
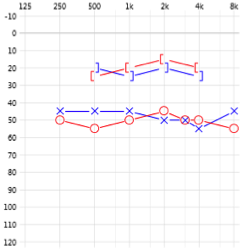
Bilateral moderate conductive hearing loss – this loss would warrant further medical investigation.
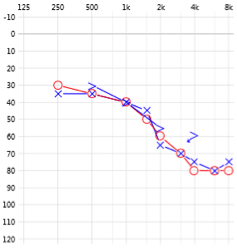
Bilateral mild to moderately severe sensorineural hearing loss – this person would benefit from hearing aids.
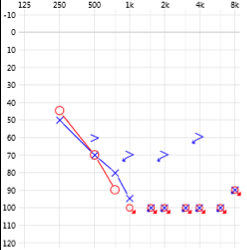
Bilateral moderate to profound sensorineural hearing loss – this client would most likely be a Cochlear implant candidate.
Note: It should be remembered that the audiogram quantitatively measures hearing; it doesn’t measure the client’s perceived quality of the sound.
TYMPANOGRAM: INTERPRETING IMPEDANCE RESULTS
Tympanometry is a test of middle ear functioning. It looks at the flexibility (compliance) of the eardrum to changing air pressures, indicating how effectively sound is transmitted into the middle ear. This objective test also allows us to view the functioning of the Eustachian Tube, the upper auditory pathways and the reflex contraction from the middle ear muscles. Impedance testing is crucial in distinguishing a conductive loss from a sensorineural hearing loss. A typical tympanometry result indicates the ear canal volume (cm3), the max pressure (daPa) and the peak compliance (ml).
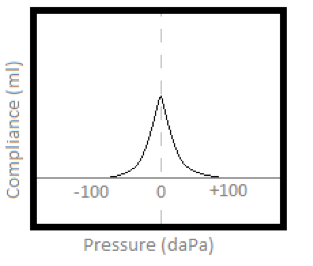
TYPE A
- Suggests normal middle ear functioning
- Peak is between +/- 100 daPa
- Compliance from 0.3-1.5 ml
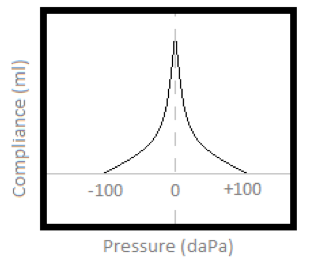
TYPE AD
- Suggests a highly compliant middle ear system
- Peak is between +/- 100 daPa
- Compliance is more than 1.5 ml
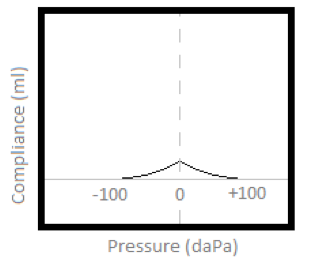
TYPE AS
- Suggests a less compliant middle ear system
- Peak is between +/- 100 daPa
- Compliance is less than 0.3 ml
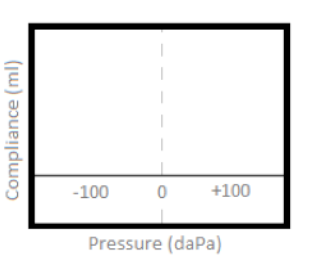
TYPE B
- Suggests middle ear involvement from fluid (middle ear effusion)
- There is no identifiable peak
- Ear canal volume is normal
TYPE B-HIGH
- Suggests middle ear involvement from a perforation or patent grommet
- There is no identifiable peak
- Equivalent ear canal volume exceeds normal limits; much larger than 1.5cm3

TYPE C
- Suggests Eustachian Tube dysfunction (often seen just before or after effusion)
- Peak is below – 100 daPa
- Compliance from 0.3-1.5 ml
OTHER REASONS FOR MEDICAL REFERRAL
Ohio Administrative Code 4747-1-19 (H)
(H) Medical referral:
A licensee should advise a prospective hearing aid user to consult promptly with a licensed physician (preferably an ear specialist) before dispensing a hearing aid to the perspective hearing aid user, and promptly document the fact that such a referral was made in the individual’s case record, if it is determined through documented case history, actual observation, or review of any other available information concerning the prospective user, that any of the following conditions exist:
(1) Visible congenital or traumatic deformity of the ear.
(2) Visible evidence of cerumen accumulation or a foreign body in the ear canal.
(3) History of active drainage from the ear within the previous ninety days.
(4) Acute or chronic dizziness.
(5) Unilateral hearing loss of sudden or recent onset within the previous ninety days.
(6) History of sudden or rapidly progressive hearing loss within the previous ninety days.
(7) Pain or discomfort in the ear.
(8) Audiometric air-bone gap equal to or greater than fifteen decibels at five hundred, one thousand, and two thousand Hertz.
(I) Except as noted in paragraph (J) of this rule, a licensee shall not sell a hearing aid unless the prospective user has presented to the licensee a written statement signed by a licensed physician that states the patient’s hearing loss has been medically evaluated and the patient may be considered a candidate for a hearing aid. The medical evaluation must have taken place within the preceding six months.
(J) An exception to medical referral can be made only if the prospective hearing aid user is eighteen years of age or older and following viewing of the ear canals, taking a case history and completing appropriate testing. The licensee may, in such cases, afford the prospective user an opportunity to waive the medical evaluation provided that the licensee:
(1) Informs the prospective user that the exercise of the waiver is not in the user’s best health interest;
(2) Does not in any way actively encourage the prospective user to waive such medical evaluation